
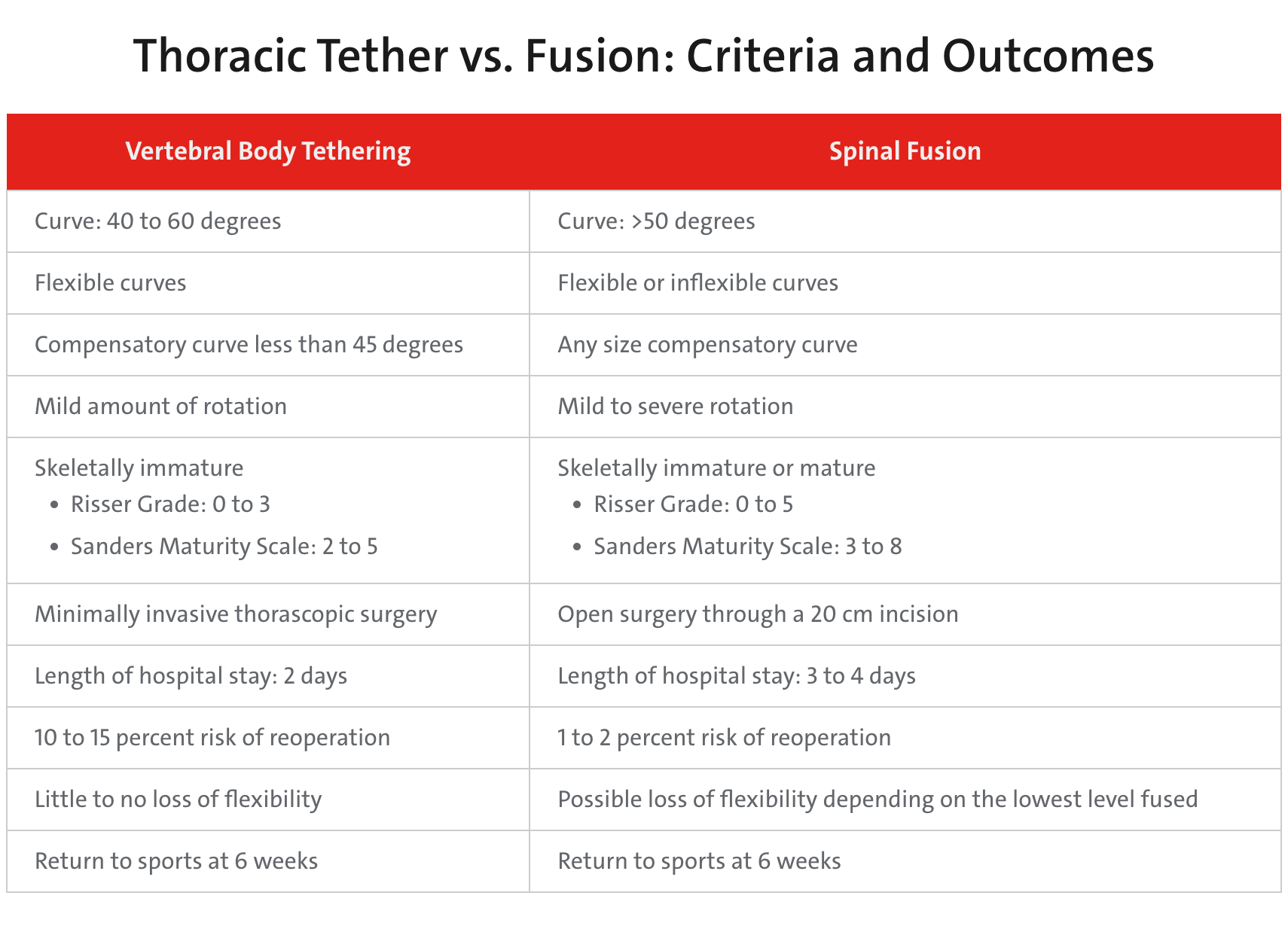
In 2019, the Food and Drug Administration approved anterior vertebral body tethering for patients with adolescent and idiopathic scoliosis who have growth remaining as an alternative to the standard treatment – posterior spinal fusion and instrumentation. In the tethering procedure, vertebral body screws and a flexible tether are placed laterally from a thoracoscopic or thoracotomy approach into the vertebral body on the convex side of a spinal deformity. A tensioning cord is secured to the vertebral body screws with set screws to connect the levels of the construct. The device provides a lateral tension band across the convex side of the spine that, on insertion and tensioning, partially corrects the curvature, and subsequently can arrest or correct the deformity through modulation of remaining spinal growth.
“I have been heavily involved with the development of tethering and have also been involved with clinical research of this procedure,” says Michael G. Vitale, MD, MPH, Chief of Pediatric Spine and Scoliosis Surgery in the Department of Orthopedic Surgery at NewYork-Presbyterian/Columbia University Irving Medical Center and the Ana Lucia Professor of Pediatric Orthopedic Surgery and Neurosurgery at Columbia. “It has been gratifying to watch this develop and also to understand the true outcomes and potential of this growth modulating, non-fusion technique.”
Dr. Vitale guides patients and their parents through the decision-making process as to which approach might be appropriate in correcting their curvature. “Both of these techniques have advantages and disadvantages,” says Dr. Vitale, who specializes in the non-operative and operative treatment of complex pediatric scoliosis, kyphosis, and adolescent Idiopathic scoliosis, performing some 200 scoliosis procedures every year. “I see my role not as a medical dictator, but as an aggregator of information for the families. Many of my patients are coming to me for a second opinion. Many are quite medically literate, and I get to act as a filter for the available information to these patients.”

“I feel that the tether does need to be an option for some patients,” continues Dr. Vitale. “As a case in point, some years ago one of my patients had a traditional fusion surgery. Then her sister developed scoliosis and opted for a tether. They have both done very well. For surgeons like myself whose practice is 100 percent in pediatric scoliosis, I believe we need to have it in our armamentarium as an offering to patients with appropriate indications and transparency about all aspects of this approach.”