
 What is it?
What is it?
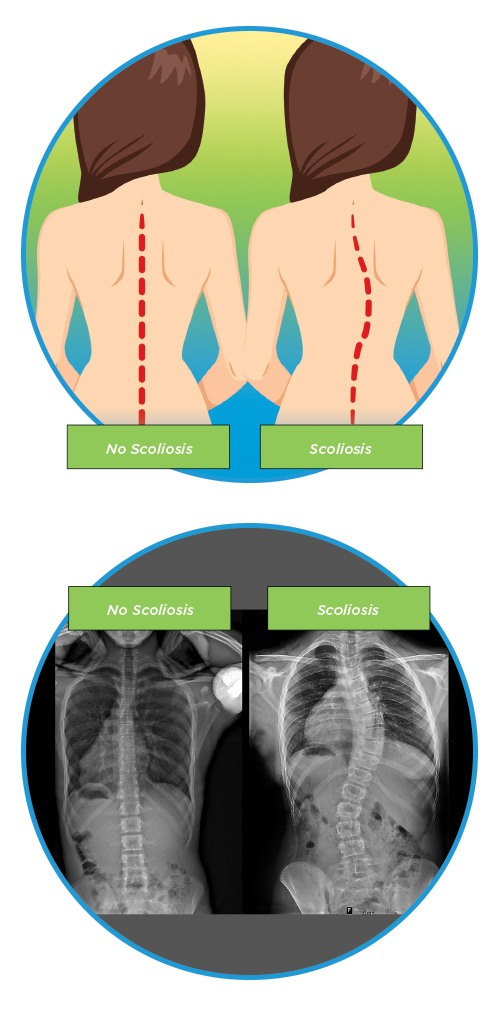
Adolescent idiopathic scoliosis, also called AIS, is a condition that affects children between the age of 10 and young adulthood and is characterized by the presence of an abnormal curve of the spine to the right or the left in the shape of an S or a C. Adolescents with scoliosis are generally healthy. Most are completely active, despite the curvature in the spine. AIS is by far the most common type of scoliosis and as many as 4 percent of all children between 9 and 14 years old have detectable scoliosis. Girls, or young women, are at higher risk than boys, or young men, with 60 to 80 percent of all cases occurring in females. AIS is often seen by the pediatrician or during a school screening at the beginning of puberty or during a growth spurt. AIS is also the type of scoliosis with the best chance of not developing a worsening curve, which is why treatment usually begins with observation only.
Some basic facts about AIS
- Scoliosis is technically defined by the presence of a curve in the spine to the right or left of >10 degrees
- While AIS is more common in adolescent girls than boys, the presence of small curves is actually equally common in boys and girls. However, many more adolescent girls than adolescent boys have severe curves, suggesting that the condition may be more likely to progress in girls.
- The incidence of the AIS is higher in children with a positive family history (i.e. a family relative also had/has scoliosis).
- Adolescents with small curves usually do not experience pain from AIS. When curves become larger or progress quickly, it can cause some back pain for patients. If there is back pain present then sometimes more tests are done to rule out any other spinal conditions or other possible causes for the pain. We may also prescribe physical therapy to help with the back pain. Most of the time, back pain is due to other things in life such as heavy backpacks, bending over books/computers/gaming systems or other various things.
What causes it?
The exact cause of AIS is unknown which is why it is called idiopathic. There has been a considerable amount of medical research that has gone into understanding scoliosis which has led to the acceptance of several hypotheses for how AIS may develop.
One possible cause of developing AIS is simply inheritance from a gene passed through a relative. The degree to which the genes end up affecting an individual is quite unpredictable. Research has suggested that several sites on more than one chromosome may be involved in the development of scoliosis. Another hypothesis gaining greater acceptance is that scoliosis is not one condition, but actually a number of different conditions, with the same clinical presentation. Each of these conditions may also have a different prognosis. This might explain the wide range of curve severity and rates of curve progression between different patients.
Much about AIS remains to be discovered and fully understood. As a result, there is ongoing research at a number of academic medical centers throughout the U.S., attempting to further unlock these medical mysteries and improve the treatment and prevention of scoliosis.
How is it diagnosed?
Adolescent idiopathic scoliosis is usually first suspected during a standard physical examination by a pediatrician or primary care physician, or during a screening test at school. Such examinations have the child or adolescent bend forward at the waist until the spine is parallel with the floor, while the physician observes the shape of the spine as it bends. If scoliosis is present then when the child or adolescent bends forward, the abnormal rotation of the spine will create a rib hump where the ribs on one side stick out slightly. If a rib hump or sign of scoliosis is found then a standing x-ray series is recommended to make a definitive diagnosis of scoliosis. As mentioned before, this requires the presence of a curvature angle of at least 10 degrees.
If scoliosis is found then you will be referred onto a Pediatric Orthopaedic Surgeon to hear about the different treatment options that are available.
A neurologic exam of the back and extremities will be performed during the physical exam and sometimes with additional diagnostic testing to make sure that no other spinal conditions are present and that the spinal cord is not being affected by the presence of the abnormal curvature.
How is it treated?
Decisions regarding the appropriate treatment for AIS depend mostly on 2 factors: the severity of the spinal curvature and the physical maturity of the patient. Because different children grow at different rates and experience growth spurts at different ages, the age of the patient is not as important as the child’s bone age. Bone age and amount of growth left can be determined by looking at the pelvic bone on x-rays (Risser grade) and hand xrays (Sanders Score). Also, because growth patterns in girls and boys tend to be different, the sex of the patient plays a role in treatment as well.
The majority of children or adolescents will have mild curves (10-25 degrees) when AIS is first diagnosed, and will therefore be treated with observation only in most cases. This means that the child will be seen regularly by a Pediatric Orthopaedic Surgeon, who will monitor the possible progression of the curve with several standing x-rays over time. The spinal curves of most children do not progress, and no further treatment is needed. However, if the curve becomes more severe, the patient may require bracing treatment.
There is a type of scoliosis specific physical therapy called Schroth physical therapy or Physiotherapeutic Scoliosis-Specific Exercise (PSSE). This may be started prior to bracing or in conjunction with bracing. Read more about Schroth Physical Therapy.
Physically immature patients with moderate curves (between 25 and 40 degrees) generally require treatment with a brace. Girls are physically immature if they are premenarchal (i.e. have not had their first period). Boys will usually receive bracing at slightly older ages than girls, because the growth of their spine continues at older ages than girls. One goal of bracing is to begin treatment before the spinal growth period is completed. There are different types of braces and you can find more information in our Scoliosis Bracing section.
With adherence to the bracing schedule, the bracing treatment is extremely successful. However, inevitably in some patients, the curve worsens, and surgery becomes the best treatment option.
In very specific situations, Anterior Vertebral Body Tethering (AVBT) is an option for patients. This is a surgical intervention to try and prevent the need for a full spinal fusion and instrumentation. Read more about Anterior Vertebral Body Tethering (AVBT).
Physically immature patients with severe curves (>40 degrees) are at a high risk of even further curve progression, and therefore usually require surgical treatment after the curve reaches 50 degrees. Curve progression is more unpredictable in physically mature patients, but if the curve reaches >50 degrees, surgery is also recommended for these patients. Scoliosis surgery in adolescents/adults consists of spinal fusion, in which the vertebrae are fused together with bone grafts and instrumentation. The instrumentation consists of metal rods that are attached to the spine to maintain curve correction. Most spinal fusions are performed through a posterior approach, in which the operation is performed with an incision in the back. The alternative is an anterior approach which is done in certain situations. This requires making an opening in the chest wall to reach the front part of the spinal column. Surgeries utilizing the anterior approach have changed in the last decade or so with the advent of thoroscopic spine surgery, in which smaller openings are made and special cameras are used to visualize the spine. This minimizes scars and recovery time. Because of the stability and effectiveness of the devices used in these spine operations today, patients are usually able to walk the day following their surgery, and hospital stays are generally about 3-5 days. The majority of adolescents returns to school within 4 weeks and can often return to full athletic activity within 6 months. Learn more information about Spinal Fusion and Instrumentation.
Resources
- App: Scoliosis Tracker for iPhone and iPad
- Book: Scoliosis: A Guide for Parents and Families
- Book: What to Expect: Conservative Scoliosis Care
- Sanders Score
- Predicting Prognosis with Sanders Score
- Predicting Prognosis with Risser Score
- National Scoliosis Foundation
- Scoliosis Research Society
- Setting Scoliosis Straight
- Curvy Girls Support Group
- SHIFT scoliosis
- http://www.iscoliosis.com
- Scoliosis Quarterly